

Neighbourhood Care Across Scotland – What Next?
On 20th March the Living Well in Communities team held a national event in Glasgow to mark the end of the first phase of the Neighbourhood Care Programme. It was an opportunity for those involved in the ihub’s national programme of work to come together with other regions in Scotland (and the rest of the UK) that are developing and testing similar models of care. 91 people attended and the roles and organisations present on the day are represented in the two word clouds below.
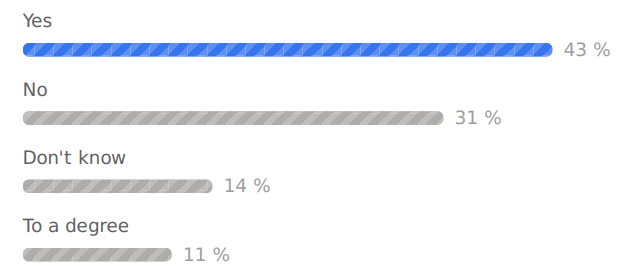
What is your job role? (n=68)

![]()
On reflection, an opportunity for improvement would be to facilitate the attendance of more of those directly involved in a care giving role.
What organisation are you representing today? (n=72)

![]() There was really good representation from a variety of organisations from all over the U.K. An opportunity for improvement would be to have more representatives from third sector and trade union organisations.
There was really good representation from a variety of organisations from all over the U.K. An opportunity for improvement would be to have more representatives from third sector and trade union organisations.
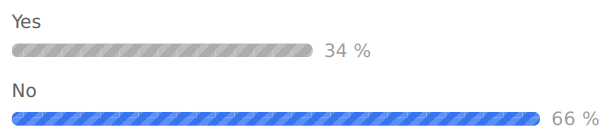
It was particularly interesting to learn that those attending had varied knowledge and experience of Neighbourhood Care in their own areas, with just over half of attendees reporting that Neighbourhood Care teams were currently operating in their place of work.
Are there Neighbourhood Care teams currently operating in your organisation? (n=35)
![]()
This poll was over lunch time and responses were lower than other polls.
The aims of the day were:
- Meet, network, share and learn from each other and leave with an improved awareness of models of Neighbourhood Care and similar activity being tested throughout Scotland
- Consider how the learning and challenges in adopting models of Neighbourhood Care can inform the design and working of integrated health and social care teams of the future
- Consider the implications for future local / national policy
The full agenda can be found here, and the slides that were used on the day can be downloaded from the Neighbourhood Care Knowledge Hub (Khub) website. You will have to become a member of the Khub website first before following this link and downloading these, but we’d encourage you to join, as we hope that this website will become a platform for those from different health and social care backgrounds to network, chat and also share resources, experience and data. Just ‘request to join’ online by following the link above, ‘sign up’ and searching for Neighbourhood Care on the Knowledge Hub, but if you have any difficulty, please contact the team on hcis.People-LedCare@nhs.net.



The audience participation tool, ‘Slido’ was used for delegates to ask questions throughout the day and to engage with each other. It was new for the majority, but most people mentioned that they liked using it in their evaluation forms, so we look forward to using it more at future events.
Have you used Slido/similar before? (n=59)
In the first part of morning, we heard from a variety of presenters in national roles: Chris Bruce, National Advisor, Neighbourhood Care Programme, Maria McIlgorm, Professional Advisor, CNOD, Scottish Government, Joanna MacDonald, Chief Officer, Argyll & Bute HSCP, and Jane Johnstone, Professional Social Work Adviser, Scottish Government.
They discussed what Neighbourhood Care meant in Scottish/integrated care context. We then heard from a mixture of sites from all over Scotland that are implementing models of Neighbourhood Care in their Health and Social Care Partnerships (HSCPs). This included South Lanarkshire HSCP, Greater Glasgow & Clyde HSCP, Angus HSCP, Cornerstone, Aberdeen City HSCP, Western Isles HSCP, Clackmannanshire & Stirling HSCP, NHS Highland and Argyll & Bute HSCP.
Generally it was acknowledge that there is definite merit in working in this way both for staff and people that receive care, but there are common challenges too.


After lunch, delegates had the opportunity to discuss the top five voted questions in the room and then the ‘barriers’ and ‘enablers’ to delivering models of neighbourhood care in different settings (with a particular focus on ‘what are the current/required solutions?’) as part of a world café session.
The engagement in these conversations was really worthwhile and produced a lot of valuable intelligence that will help guide the future national direction of this programme of work.
As there wasn’t enough time on the day to answer all the pertinent questions posted on Slido, the LWiC team decided to pose these questions to the most appropriate individuals/teams and collate the responses. Thank you to all who have provided the questions and the answers. The response document can be found by following this link.




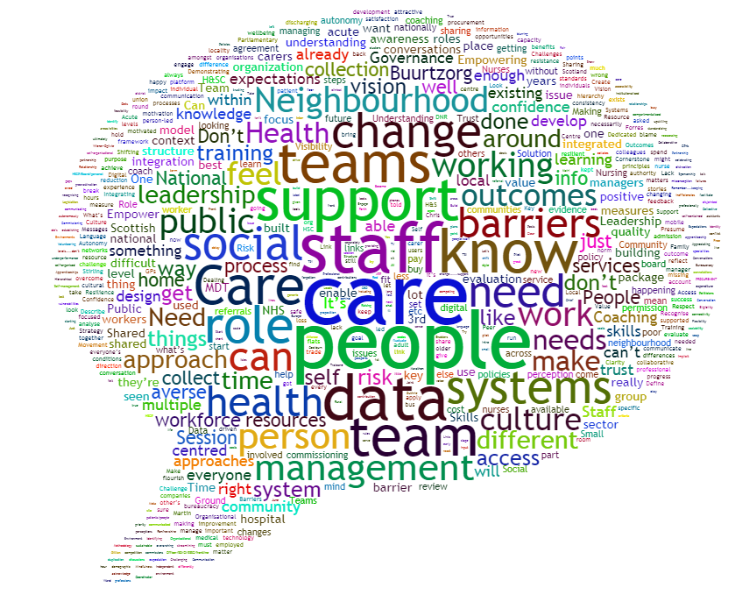
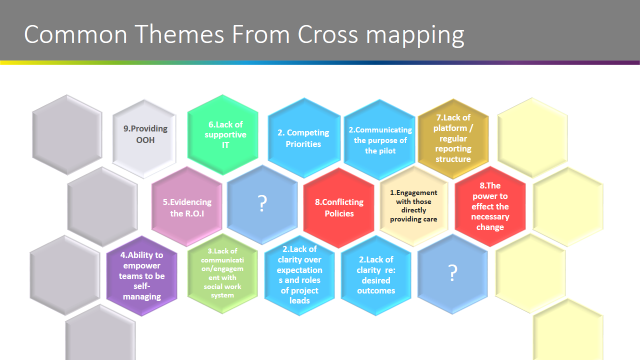
The world café session provided information that was particularly useful. The full transcription of the flipchart notes from the twelve individual tables is here, but the world cloud below that has been generated from combining all discussions highlights the key themes really well.
Within the Healthcare Improvement Scotland’s Improvement Hub (ihub), the Neighbourhood Care programme will move from the Living Well in Communities (LWiC) team to the Person-Led Care team from April 2019 as it enters a second phase. Chris Sutton, Portfolio Lead for the Person-Led Care team, introduced herself to the room on the day and will use the outputs from these valuable discussions to inform the future actions needed to support the delivery of the Neighbourhood Care Programme going forward. For any further information or to find out how you and your team can engage, please contact the Person Led Team on: hcis.People-LedCare@nhs.net.
 Fiona McQueen, Chief Nurse, Scottish Government rounded off the day with her reflections. Fiona discussed the great impact stories that were shared earlier in the day and stressed that working together in an integrated manner is the only way to provide truly person-centred and holistic care.
Fiona McQueen, Chief Nurse, Scottish Government rounded off the day with her reflections. Fiona discussed the great impact stories that were shared earlier in the day and stressed that working together in an integrated manner is the only way to provide truly person-centred and holistic care.
‘We still have a long way to go, but it’s a very worth-while journey’
Thank you to everyone who attended. Here are a few short ‘Vlogs’ that captured your general experience and learning on the day.
Future general enquiries/information requests should be directed to hcis.People-LedCare@nhs.net











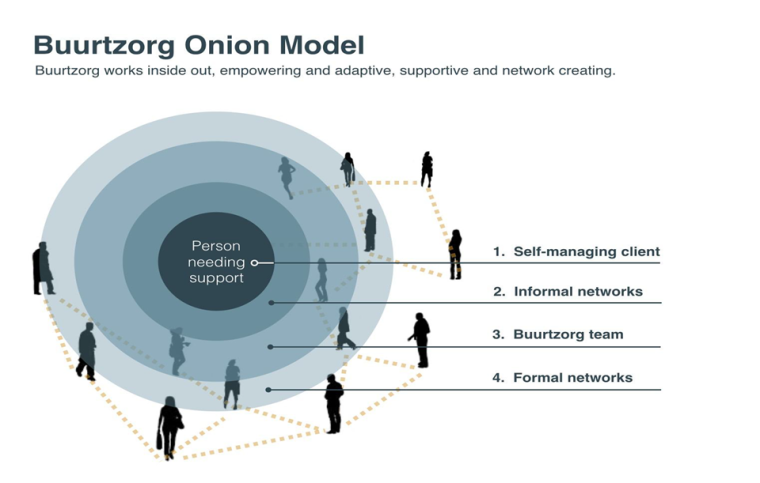





 I would like to take the opportunity to introduce myself as the Programme Manager with Healthcare Improvement Scotland, responsible for coordinating the work on applying the principles of Buurtzorg to develop Scottish models of neighbourhood care.
I would like to take the opportunity to introduce myself as the Programme Manager with Healthcare Improvement Scotland, responsible for coordinating the work on applying the principles of Buurtzorg to develop Scottish models of neighbourhood care.